Why pre-surgical 3D planning is underused
There is widespread clinical consensus that 3D anatomical models improve surgical planning. A surgeon who has walked through the patient-specific anatomy before making an incision — identifying unexpected vascular variants, understanding exact organ relationships, planning approach angles — is better prepared than one working from 2D slices alone.
The obstacle has never been the value of 3D planning. It is the cost of producing the models. In a traditional workflow, someone has to manually trace organ and tissue boundaries, slice by slice, on axial, sagittal, and coronal views. For a complex abdominal CT with multiple structures of interest, that is 4 to 8 hours of skilled operator time. At that cost, 3D planning gets reserved for the most complex cases — and many departments do it for none of them.
The constraint was never clinical usefulness. It was operator time. AI segmentation removes that constraint, making 3D planning accessible for routine complex cases rather than exceptional ones only.
What AI segmentation actually does
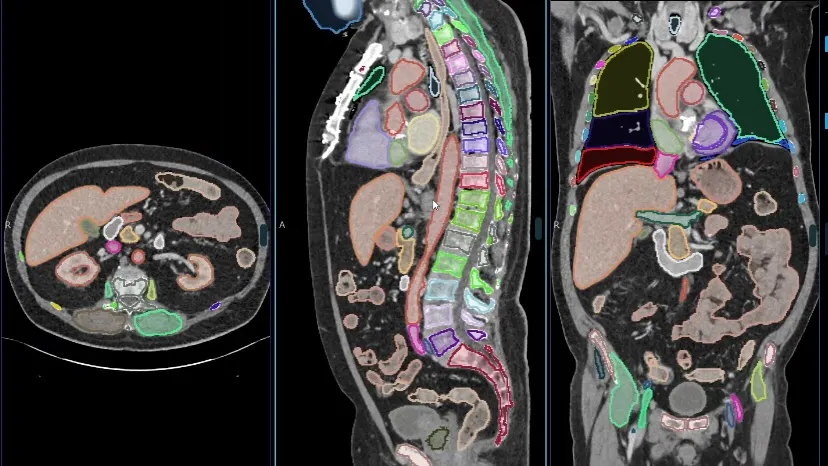
Modern organ segmentation systems use deep convolutional neural networks trained on large, annotated imaging datasets — typically hundreds of thousands of manually contoured volumes from diverse patient populations. The model learns to identify each anatomical structure based on intensity patterns, spatial relationships, and contextual cues across the full 3D volume.
The output is a set of contoured volumes — one per structure — stored as masks that can be rendered in 3D, exported in various formats, or overlaid on the original imaging data. For a whole-body CT, this means 117 or more individual anatomical structures simultaneously contoured in a single automated pass.
Importantly, this is not the same as segmentation-by-thresholding (which has been available in radiology workstations for decades and produces noisy, disconnected results). Deep learning segmentation produces smooth, anatomically accurate contours that correspond to how a trained clinician would manually delineate each structure — because that is exactly the data the model was trained on.
The full workflow: DICOM to surgical model
Here is what the end-to-end workflow looks like with AI segmentation integrated into a radiology department:
DICOM series arrives from scanner or PACS
The CT or MRI volume is sent to the segmentation system — either pushed from the PACS automatically or uploaded manually. No conversion required; native DICOM is the input format.
AI model runs segmentation on the full volume
The deep learning model processes the 3D volume and generates contour masks for each relevant anatomical structure. For a standard abdominal CT this takes 5–15 minutes depending on volume size and server hardware.
Results reviewed and adjusted if needed
The radiologist or physicist reviews the generated contours in the viewer. Minor corrections can be made to individual structures. In the majority of cases on standard anatomy, the AI output is used directly.
Export in the required format
The contoured volume is exported as DICOM-SEG (for PACS archiving), STL or OBJ (for 3D printing), glTF (for AR/VR and surgical simulation), or NIfTI (for research and downstream analysis).
Where the output goes: use cases by format
STL and OBJ — 3D printing for pre-surgical models
Patient-specific anatomical models printed in resin or FDM plastic are used by surgical teams to understand complex anatomy before the patient is on the table. Orthopaedic surgeons use bone models to plan implant positioning. Hepatobiliary surgeons use liver and vascular models to plan resection margins. Paediatric cardiac teams use heart models for complex congenital cases.
Without AI segmentation, the cost of producing a 3D-printed surgical model for a routine case was prohibitive. With it, the bottleneck is the printer, not the operator.
glTF — AR/VR and surgical simulation
glTF is the standard format for real-time 3D rendering — it loads directly into surgical simulation platforms, AR headsets, and VR environments. Surgeons can walk through a patient-specific anatomy in virtual reality before performing a procedure, or overlay the 3D model onto the actual patient via augmented reality during surgery. This is already in clinical use at large academic medical centres; AI segmentation makes it accessible to district general hospitals and regional cancer centres.
DICOM-SEG — PACS round-trip and longitudinal tracking
DICOM-SEG exports the segmentation results in a format that loads back into any DICOM-capable PACS, alongside the original imaging data. This matters for oncology departments tracking tumour volume over treatment cycles — each follow-up scan generates a new segmentation, and the PACS maintains the full longitudinal record.
Accuracy: what to expect and what to ask
AI segmentation accuracy is typically reported as Dice Similarity Coefficient (DSC) — a measure of overlap between the AI-generated contour and a reference manual contour. For well-defined organs like the liver, kidneys, and spleen, state-of-the-art models routinely achieve DSC above 0.92 on external validation datasets. For smaller or more variable structures, accuracy is lower.
When evaluating any segmentation system, ask for validation data specifically — not just training data accuracy. Training accuracy is not informative. External validation on a dataset the model has never seen, from a different institution, is what predicts real-world performance. Ask which structures are included in the validation, the patient demographics, and how performance degrades on pathological anatomy.
No AI segmentation system is a substitute for clinical review. The workflow is: AI produces the initial contours, a trained clinician confirms or corrects them. What changes is where the operator's time goes — from drawing contours to reviewing and refining them. That is a 10x reduction in time, not a removal of clinical responsibility.
Key takeaways
- Manual CT segmentation for surgical planning takes 4–8 hours per case; AI reduces this to under 20 minutes.
- AI segmentation uses deep learning models trained on large annotated datasets — the output is anatomically accurate, not thresholded.
- The workflow is: DICOM in → AI contours generated → clinician reviews → export in required format.
- Export formats serve different use cases: STL/OBJ for printing, glTF for AR/VR, DICOM-SEG for PACS, NIfTI for research.
- Evaluate any tool on external validation DSC data, not training accuracy. Ask specifically about the structures and patient populations in the validation set.
- AI produces the initial contours; clinical review remains essential.